
This second case report is actually a guest post by a fellow-in-training with the Institute of Physical Art’s (IPA) fellowship program in New York City. The author is YJ Cho PT, DPT, CFMT. YJ wrote this case report as part of a “Clinical Pearl” segment for the IPA’s google group. After reading it, I thought it would be a great case to share with all of you, so enjoy!
Referred Pain Case Study
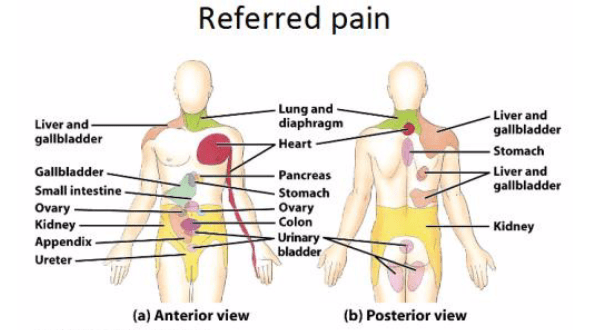
The neuroanatomic and physiologic theories that explain the phenomenon of referred pain is widely accepted by multiple health care disciplines. It is highlighted in musculoskeletal classes as well as pathology classes linking the different systems of the human body. However, in clinical practice, it is often forgotten but more importantly, there is a lack of agreement amongst different disciplines on how to effectively treat referred pain. Some prefer medications, surgical removal of the “non-vital” organs, or perhaps a more holistic route like acupuncture, herbal medicine, or a strict dietary modification. Manual therapy is slowly being considered but still is not widely understood or accepted by health care professionals including physical therapists. Below is a case study of a patient that was successfully evaluated and treated utilizing Functional Manual Therapy for a visceral referred pain.
Brief History:
Patient is a 69-year old male with chief complaint of discomfort that is described as diffused and vague around the entire lower 2/3 of the abdomen. He reports that this sensation goes all the way into his groin and it can also be felt around his testicles. This sensation has been progressively worsening for the past 4-5 months. Through additional questioning, he also notes that he has been in and out of outpatient physical therapy for the past 2 years with R>L sided mid/low back pain that has not gotten better. He notes that it is the worst in the morning when he wakes up (supine/sidelying sleeper) and typically gets better as the day goes on. He describes this pain as heavy pressure and achy. Upon further questioning, he reports that it is extremely uncomfortable when his bladder fills up with fluid. He notes that because of this discomfort, there is an urgency to get to a bathroom and urinate as quickly as possible. He reports that the act of urination is not painful.
Medically, he has seen multiple medical doctors on different occasions including his primary care physician, spine specialist, and a urologist. No significant findings on X-ray, MRI or CT scan. Because of the complexity of his symptoms, cancer was considered at one point secondary to a small benign mass in the pancreas and gall bladder. Cancer was still not ruled out at this point and the patient was to go further testing to confirm in upcoming weeks. Kidney stones were found in both kidneys and consideration of removal of stones have also been discussed. Lastly, ultrasound/scan of the testicles revealed a mild hydrocele and drainage of this inflammation has also been considered.
Objective Exam:
The discomfort in his mid/lower back could not be reproduced with any active or passive movement of his spine or his extremities, even with over pressure. The diffuse/vague pain in the abdomen also remained 4-5/10 on a self-reported “discomfort scale” throughout with no change during or after objective exam. No significant tension noted in slump or extension sitting testing. No pain reproduced with percussion testing of both kidneys.
Observation of movement:
-Saliba Postural Classification System reveals a posterior/anterior posture
-Noted during active range of motion: decreased excursion of rib cage from abdomen circumferentially and poor access into all parts of diaphragm during breathing. Mostly belly breathing and chest breathing.
-Gait lacks push off excursion bilaterally
Palpation:
-Significant fascia tension noted anterior abdomen and around contours of rib cage
-Palpation of mid/low back bilaterally did not reproduce pain. Notes that palpation of quadratus lumborum, paraspinals, ribs or any musculoskeletal structures around this area did not feel like the structure involved in his discomfort
Treatment:
At this point, he was supine on the table and we have been conversing further about his symptoms throughout. We have discussed that his symptoms do not exhibit the characteristics of cancer and that it was interesting that his back pain could not be palpated or reproduced with physical movement. My plan was to examine his abdomen through palpation and also explained to him that bladder seemed to be involved because of his complaint of pain when the bladder filled up. I could feel that there were layers of significant soft tissue tension along his abdomen including around his bladder and his pubic symphysis. He noted that his prostate is slightly enlarged but is being monitored carefully and no issues otherwise. I went Functional Mobilization I style working through the cascade of techniques in which he noted throughout that it was an interesting sensation but felt that there was some relief of tension around his lower abdomen. I worked through the restrictions of his bladder, localizing through his lower extremities in the jack-knife position.
Now, as I began working into the deeper layers of his abdomen, I noticed a “lump” or a thick structure in his left lower abdomen laterally. I have never felt this structure before on anyone and my immediate thought was “what is this structure and, uh oh is this a mass of some kind”? It felt thick and thick and maybe around the half way point between his ASIS and belly button. Too superficial to be his psoas major. I tried not to exhibit my concern onto the patient and tried to outline this structure through palpation. I realized the structure ran vertically and was tubular in nature. As I started palpating cranially, I could feel it was connecting into another structure that was much bigger but this structure was also restricted deep posteriorly into the rib cage. At this point, I began realizing the vertical structure was his ureter and the bigger structure that I was on was his L kidney. Understanding the structures that I was working with, I able to feel that the ureter was more restricted cranially into his kidneys vs caudally towards his bladder. I began working on improving the play of his L kidney through 3-D localization with the use of his lower legs and breathing. A lot of rotation through the trunk was needed to localize fully onto the kidneys. At one point, we both felt his kidney become softer to touch and free up from the restriction that it was adhered to. We both looked at the each other at this moment and I asked him, “did you just feel that?” in which he responded with a “yeah, yeah” and a perplexed look on his face. Furthermore, this taut band that was running vertically was 90% softer and did not have the same quality of tension to how it felt minutes prior. This is a moment that I will never forget for the rest of my life. I treated his right kidney the same way I did with his left kidney and went back to treat his bladder once more. A few hours later, I treated his psoas, anterior lumbar spine, diaphragm and mid thoracic spine with resisted breathing given as his home exercise program.
Immediately following the treatment, he noted that his discomfort in the abdomen was about 30% better but still felt “weird”. The following day, he communicated to me that he still had the diffuse/vague pain in his abdomen and groin but the back pain felt significantly better when he woke up. I was honestly hoping that his diffuse/vague pain would also be better. However, within a 10-day period with no other treatments, all of his symptoms gradually resolved including the diffuse/vague pain in his abdomen, groin and testicles, R>L back pain upon waking, and the discomfort when his bladder fills up.
Take away Points: Through my subjective questioning, I was able to focus my treatment that ultimately led to the primary problematic structures. I could be confident in my approach by ruling out major red flags and narrowing down my problem list. This skill of asking the right questions is constantly being challenged throughout fellowship. Furthermore, I must also admit that although I have taken VFM with Dean Hazama, I have yet to take any of Barral’s Visceral Mobilization classes. I also did not realize that kidney/ureter referral went to literally all the areas that he described his discomfort to be until I googled it after the treatment. Although I have some exposure to Barral’s work, I am excited about to purse and learn his work in the near future. However, for those of us that may not have extensive training in this area, by trusting our hands, being gentle and utilizing the principles of treatment taught in FM II (trace and isolate), we can still make a big impact in a complex case like this. This fellowship has also taken my ability to localize and trace/isolate to a much stronger level which was crucial in this case. Lastly, it was also a reminder to be patient with treatment results. The body heals in mysterious ways at times and it may take time for the body to take in the work that we just did and begin the healing process after being dysfunctional for so long.
I will forever remember this case because of the uniqueness in its presentation, the result of the treatment, and because this patient happened to be my father. He is currently complaint-free and my mom now loves me that much more.

Wow! Great case study.
LikeLiked by 1 person